Effectiveness of Home-based Cardiac Rehabilitation strategies for Saudi Arabia’s elderly residents living with chronic conditions during the Covid 19 epidemic
1.0 Introduction
1.1Background Information
Cardiac Rehabilitation (CR) is an intervention based on evidence which applies health behavior modification, exercise training and patient education to boost secondary curbing results in patients suffering from cardiovascular disease (CVD). Programs developed for CR practice bring down the rates of mortality and morbidity in elderly individuals who suffer from heart failure, cardiac surgery or heart disease (Haukilahti et al., 2015 p.54).. However, such programs are yet to be optimally applied. Currently the CR programs in Saudi Arabia are only applied in few cardiac patients. Therefore, new delivery strategies are needed urgently to enhance patient participation. Home-based CR is among the possible strategies. The Saudi Arabia Kingdom (KSA) is faced with ever increasing rate of mortality caused by the cardiovascular diseases (CVDs), especially among the elderly patients, as well as the prevailing rate of coronary heart disease (CHD). CHD has been found to cause many deaths from CVDs in Saudi Arabia (Thomas et al., 2019 p.34). The analysis of the data on the stated rates of epidemiology forecasts an increase of these rates which is brought about by more exposure to risk factors that cause CVDs. The American Association of Cardiovascular and Pulmonary Rehabilitation (AACVR) and the National Institute for Clinical Excellence (NICE) records that patients’ participation in phase III cardiac rehabilitation (CR) programs is can significantly reduce mortality and morbidity rates in elderly CHD patients due to Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Surgery (CABG) (Thomas et al., 2019 p.34). Unfortunately, there is no phase III offer of CR for elderly patients in KSA. This state is made worse by the emergence of the Covid-19 epidemic across the world which has made it almost difficult for governments to give healthcare services to other patients. There is a dire need to establish strategies that will be used to offer effective home-based care to patients with CVDs in Saudi Arabia (Al Muallem, et al., 2015 p.34). Therefore this study shall seek to assess the effectiveness of home-based cardiac rehabilitation strategies for the elderly patients with chronic conditions during Covid 19 pandemic.
1.2 Problem Statement
Towards the close of 2019, novel corona virus (Covid-19) which is highly infectious emerged as a world pandemic with millions of cases getting reported across the world. Since Covid-19 is a highly infectious disease affecting the respiratory system, strict measures have been imposed by various world governments to curb its spread. In Saudi Arabia, the government has imposed measures such as restricted movements or the famous “stay home” initiative. Consequently provision of Home Based Cardiac Rehabilitation for elderly patients suffering from chronic heart diseases has been greatly impacted by this pandemic. In response, strategies have been formulated to ensure that HBCR is offered to such patients. However, the home based cardiac rehabilitation programs have not yet been optimally applied especially during this period of Covid 19 pandemic.
1.3 Objectives
The research aims at assessing the effectiveness of HBCR for elderly patients in Saudi Arabia. The main objectives of this study are;
- To assess the effectiveness of Home-based Rehabilitation strategies for Saudi Arabia’s elderly residents with chronic conditions during the Covid 19 epidemic
- To highlight and discuss how the emergence covid 19 has affected the provision of Home based cardiac Rehabilitation
- To evaluate the current strategies applied in HBCR
1.4 Thesis Structure
1.4.1 Research Questions
- Are the HBCR strategies effective for elderly patients with chronic CVDs
- What is the scope of the existing HBCR strategies
- What are the impacts of Covid 19 on provision of HBCR
1.4.2 Hypothesis
- Covid 19 affects the effectiveness of provision of home-based cardiac rehabilitation (HBCR)
- HBCR strategies are effective for elderly patients with chronic Cardiovascular Diseases CVDs
2.0 Literature Review
2.1 Introduction
In spite of the rising cases of cardiovascular diseases (CVDs) among the elderly patients, apparently there is a string bias in the rehabilitation and CVDs treatment that comprise of several preventive strategies. Information contained in Ades and colleagues and many other institutions shows that CVD elderly patients are less possibly to be referred to cardiac rehabilitation programs which are formal. Even if they are referred, they usually experience very poor compliance to the programs because of lack of strong inputs on recommendations by the referring doctors. In most health institutions in Saudi Arabia, such as King Faisal Specialist Hospital and Research Center, routine referrals of elderly patients for cardiac rehabilitation are done; however, just a half of these referrals are attended frequently as compared to patients who are of younger age (Ponikowski et al., 2014). Nonetheless, a number of caregivers have reported remarkable results of “formal phase II cardiac rehabilitation and exercise-training program on obesity indexes, plasma lipids, quality of life (QOL), behavioral characteristics, and exercise capacity, comprising sub groups of elderly patients who are above 75 years of age and women who are older” (Sheehy, 2020 p.19462).
2.2 Theoretical Review
Healthcare services on cardiac rehabilitation are the major and crucial constituent in the continued care for elderly patients suffering from cardiovascular diseases (CVDs). Recommendation of the class IA, medical referrals to cardiac rehabilitation registers 1 out of 9 measures of performance for prevention (secondary) as established by the American Heart Association and American College of Cardiology following; coronary artery bypass graft surgery, percutaneous coronary intervention or myocardial infarction (MI) or symptomatic peripheral arterial disease (intermittent claudication) or in the setting of stable angina. Cardiac rehabilitation referrals are also done following cardiac transplantation, setting in of chronic heart failure (HF) with lowered ejection fraction or valve surgery. CR referrals following MI is the “defect-free care” section strategy performance involved in the Centers for Medicare and Medicaid services in the agreement core set of cardiovascular performance strategies Haukilahti et al., 2015 p.54).. The effectiveness and safety of the conventional clinically monitored, Center-based Cardiac Rehabilitation (CBCR) model are strongly founded, and CBCR is thus effective in lowering readmissions to hospitals, mortality and morbidity in elderly patients suffering from CVDs as well as secondary events (Quait et al., 2017 p. 100).
Conversely, the implementation and effect of CBCR in Saudi Arabia has been considerably slowed by significant underutilization by eligible elderly patients. Information from various databases and registries show that even though CBCR referral, talking in overall terms, is improving, participation by eligible elderly patients is still low in most of the sub-elderly groups. Participation is particularly reduced among the beneficiaries of Medicare, women and elderly persons from underserved populations such as the ones from those within the lower socioeconomic stratum, the ones who are underinsured or uninsured. Clearly state-of-the-art delivery strategies are required urgently for a bigger percentage of elderly patients in Saudi Arabia who currently do not take part in cardiac rehabilitation. Among the most promising approaches is the alternative site or popularly known home-based cardiac rehabilitation (HBCR), that can be implemented in different settings such as nonclinical settings including parks, health clubs and community centers or home setting which is the most appropriate during Covid 19 pandemic (Haukilahti et al., 2015 p.54).. Conceptually, HBCR can possibly aid in addressing most of the challenges which CBCR programs have been facing such as logistical, geographical as well as other access-related challenges. Even though home-based exercise training is usually advocated for by CBCR staff for their CVD patients during occasions when they are physically absent from the centers, outstanding HBCR programs are yet to be fully explored and strategized to effectively provide care for elderly CVD patients. Nonetheless, NICE guidelines on CVD prevention suggests “home-based cardiac rehabilitation with or without telemonitoring is promising the increment of the participation and supporting behavioral change. Additionally, Cochrane and colleagues reviews on cardiac rehabilitation have conclusively proposed that “low-to moderate-strength evidence that CBCR and HBCR” register same impacts on quality of life as well as cost among elderly patients who in the recent past were diagnosed of revascularization or MI (Haukilahti et al., 2015 p.54)..
HBCR single application or coupled with CBCR offers a potential alternative which can enhance CR provision to elderly patients in Saudi Arabia. HBCR has been integrated into the Medicare systems of many countries such as Australia, United Kingdom, Canada among others. HCBR bears many advantages including the potentiality to overcome most logistical challenges such as scheduling barriers and transportation, which have been main challenges in programs of CBCR. Moreover, it has the possibility of expanding the depth and breadth of counseling, educational as well as monitoring of opportunities for elderly patients since HBCR services cab likely be used throughout (Thomas et al., 2019 p.34). In contrary CBCR programs are normally time-bound – about 3 to4 hours in a week. Since most elderly patients with CVDs take more than 5000 hours walking every year, without the help of health workers, it is crucial to equip them with behavioral change strategies which can be done in their home as well as community environments. Nevertheless, HBCR implementation encounters considerable challenges in Saudi Arabia; most noteworthy is a deficient reimbursement by the Centers of Medicaid and Medicare services as well as tertiary players. Interestingly, a recent research on the CR-eligible elderly patients indicates that most of them prefer home-based than Centre-based approach (Montgomery et al., 2013 p.65).
2.3 Empirical Review
Lavie and Milanie (2004), state that the major common symptom among the elderly patients with CVD events is depression with a point prevalence of 18%. Such elderly patients experience lower HDL levels, lower QOL scores somatization, hostility and reduced exercise capacity. When cardiac rehabilitation was carried out in these patients, they registered a 57% lowering of the prevalence of depression scores (p<0.0001) and more than 32% boosts in their quality of life scores and also recorded enhancements in exercise “capacity, HDL as well as other CVD risk factors (p 33). Even though elderly is commonly defined as more than 65 years, most health experts concur that most of the patients between 65 and 75 years are somehow young, less information is available for extremely elderly patients. CVD patients who are very elderly going home-based cardiac rehabilitation have been found to register improvements to significant levels of plasma lipids, such as summed cholesterol (-5%; p=0’01), low-density lipoprotein (LDL) cholesterol (-6% p = 0.04) HDL (+6%; p = 0.05), triglycerides (-16%; p<0.001), as well as a LDL/HDL ratio (-8%, p = 0.02) and also gradual improvements in approximated exercise capacity (+39%; p = 0.00001). Such improvements showed to be more in elderly patients (Sipilä et al., 2019 p. 300)
Elderly patients with chronic CVD conditions, especially elderly women, are possibly the rapidly growing portion of the population in society and in health practices of cardiovascular, this segment of the society is likely going to be the least referred to and be provided with cardiac rehabilitation programs. For many parameters, boosts after cardiac rehabilitation are statistically same in the elderly patients as compared to other patients. Nonetheless, elderly patients have recorded great improvements in obesity indexes due to home-based cardiac rehabilitation such as body mass index (-2% vs 0%; p < 0.03), percentage of body fat (=10%; -5%; p < 0.01). The boosts in the weight of the body are specifically remarkable because obesity is apparently the strongest risk factor in elderly women. Various literature based performed experiments support the positive results of strength training and aerobic exercise training in generally enhancing quality of life and physical fitness. Notably, elderly patients taken through particular strength training enhanced their upper extremity strength, social QOL as well as physical QOL. In deed support strength training and physical exercises points to the effectiveness of home v=based cardiac rehabilitation (Haukilahti et al., 2015 p.654). The major segments of HBCR found to be effective with elderly patients with CVD include; dietary counseling, exercise training, patient education and assessment, behavioral activation such healthy eating habits, physical activity and smoking cessation, risk factor control including hypertension, diabetes mellitus, obesity and lipid abnormalities as well as psychological interventions. Such intervention components can easily be implemented at home even in the absence of monitoring by health care providers (Haukilahti et al., 2015 p.654).
-
- Conceptual Framework
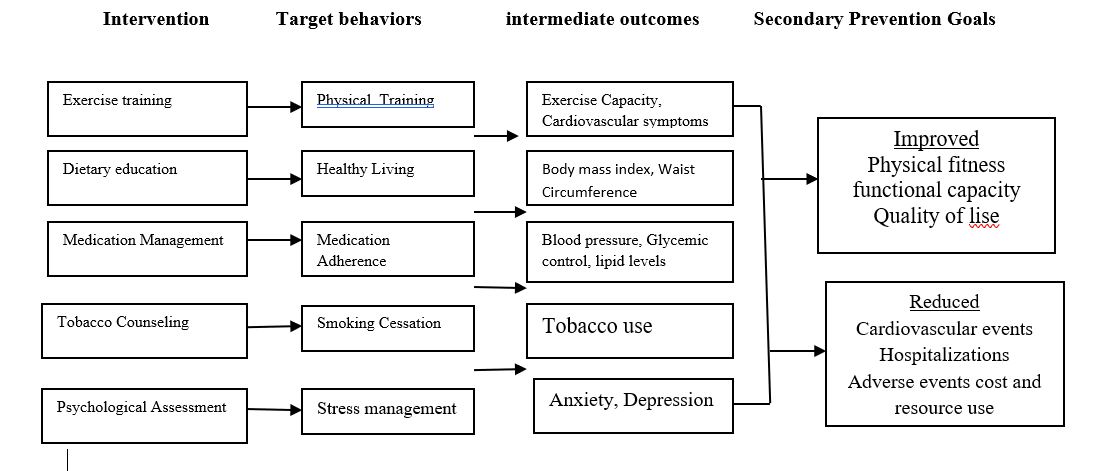
2.5 Summary
The discovery that cardiac rehabilitation services, especially can safe lives and yet they are underutilized points to the urgent need of coming up with new approaches to supplement the provision of CR services. Generally, effectiveness of HBCR is attributed to various components. Interventions constituting dietary counseling, exercise training, psychological support, weight management lipid management and blood pressure management as well as healthy lifestyle, have been established to greatly enhance the QOL of elderly patients with CVDs. However, determination of most beneficial and the best components of the HBCR interventions is made difficult by the length and intensity of the program, patient characteristics as well as the delivery mechanisms. HBCR offers a promising alternative option in provision of CR services for stable low-to moderate risk elderly patients with CVD especially in this period of Covid 19 pandemic.
3.0 Methodology
Research methods refer to the techniques and tools utilized in carrying out a research and a range of tools which are applied for various enquiry types. Different research methodologies are available including qualitative, quantitative as well as mixed methods
3.1 Design
This research will utilize a qualitative research design through collection of primary data. The selected participants will be requested to voluntary give their experiences which relate to their feelings of the provision of home based cardiac rehabilitation particularly after the onset of Covid 19 pandemic. Such experiences shall be collected, documented and eventually subjected to analysis. The research participants will comprise of CVD elderly patients, health care providers as well as administrators. In addition, researcher’s experiences acquired through participatory observation will also be considered for analysis.
3.2 Setting
The research shall be conducted in respective homes and community centers where CVD elderly patients are residing in Riyadh and its environs. The city of Riyadh hosts several elderly patients with CVD and the number keep increasing as indicated in the world health organization (WHO) database. Such numbers, although spread likewise across the world, are becoming more prevalent in Saudi Arabia and especially in Riyadh. This renders the city a percent study area for this research.
3.3 Sampling
Purposive sampling technique will be adopted by this research. The researcher shall judge who to participate among the elderly CVD patients in their various homes or in a community center. Various homes and community centers will be identified and then the researcher shall visit the identified places and select the participants.
3.4 Research Instruments
A questionnaire which is well structured shall be used as an instrument for gathering primary data. The questionnaire will comprise of two sections. The first section is for entering the demographic data of the respondents such as Sex, Age and years with CVD. The section is crucial because it will give the age of the participants and indicate how long the patient has been suffering from CVD. The other part will consists of different research questions framed to provoke responses on the experiences related to the effectiveness of home based cardiac rehabilitation strategies since the onset of Covid 19 pandemic.
3.5 Data Collection Procedure
Various means can be employed in collecting primary data such as online distribution of questionnaires, hand delivery as well as using google documents. This research project shall opt for the use of hand delivery means since the participants are mostly elderly people hence need of personal touch. Filled up research questionnaires from respondents will be picked with the help of research assistants. The responses will be cleaned, documented and subjected to analysis.
3.6 Data Analysis
The collected data shall be subjected to descriptive data analysis mode of evaluation. The data, after collection, shall be coded and entered into software for analysis. In particular SPSS data analysis will be opted for and then the data will be translated into such measures of variability as skewness, kurtosis, and central tendency.
3.7 Ethical Considerations
Research ethical considerations will be considered during the conduct of the research. Such considerations shall include upholding the confidentiality of every personal detail of the participants. In addition, the participants will be informed concerning their consent before participating. The aim and the objective of the study will be made known to the participants and their freedom to choose to participate and withdraw before and during participation. Lastly, every crucial approvals and licenses shall be sought and any fee required shall be given out before the onset of this research.
References
Al Muallem, Y., Al Dogether, M., Al Assaf, R., Al Ateeq, A., Al Moammary, E., Al Ghamdi, H. and Househ, M.S., 2015, July. Remote Patient Monitoring System Implementation at a Cardiac Care Centre in Saudi Arabia. In ICIMTH (pp. 33-36).
Haukilahti, M.A.E., Eranti, A., Kenttä, T. and Huikuri, H.V., 2016. QRS fragmentation patterns representing myocardial scar need to be separated from benign normal variants: hypotheses and proposal for morphology based classification. Frontiers in physiology, 7, p.653.
Lavie, C.J. and Milani, R., 2004. Benefits of cardiac rehabilitation in the elderly. Chest, 126(4), pp.1010-1012.
Mahmood, D., Jahan, K. and Habibullah, K., 2015. Primary prevention with statins in cardiovascular diseases: A Saudi Arabian perspective. Journal of the Saudi Heart Association, 27(3), pp.179-191.
Montgomery, S.R., Zhang, A., Ngo, S.S., Wang, J.C. and Hame, S.L., 2013. Cross-sectional analysis of trends in meniscectomy and meniscus repair. Orthopedics, 36(8), pp.e1007-e1013.
Ponikowski, P., Anker, S.D., AlHabib, K.F., Cowie, M.R., Force, T.L., Hu, S., Jaarsma, T., Krum, H., Rastogi, V., Rohde, L.E. and Samal, U.C., 2014. Heart failure: preventing disease and death worldwide. ESC heart failure, 1(1), pp.4-25.
Quait, A., Mohamed, A.I. and Doherty, P.J., 2017. Overview of cardiac rehabilitation evidence, benefits and utilisation. Global Journal of Health Science, pp.38-48.
Sheehy, L.M., 2020. Considerations for Postacute Rehabilitation for Survivors of COVID-19. JMIR Public Health and Surveillance, 6(2), p.e19462.
Sipilä, R., Mikkelsson, M., Honkanen, M., Malmivaara, A. and Komulainen, J., 2019. Development and Application of Implementation Tools for Rehabilitation Guidelines. Journal of rehabilitation medicine, 51(11), pp.834-840.
Thomas, R.J., Beatty, A.L., Beckie, T.M., Brewer, L.C., Brown, T.M., Forman, D.E., Franklin, B.A., Keteyian, S.J., Kitzman, D.W., Regensteiner, J.G. and Sanderson, B.K., 2019. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Journal of the American College of Cardiology, 74(1), pp.133-153.
